Understanding Peyronie’s Disease
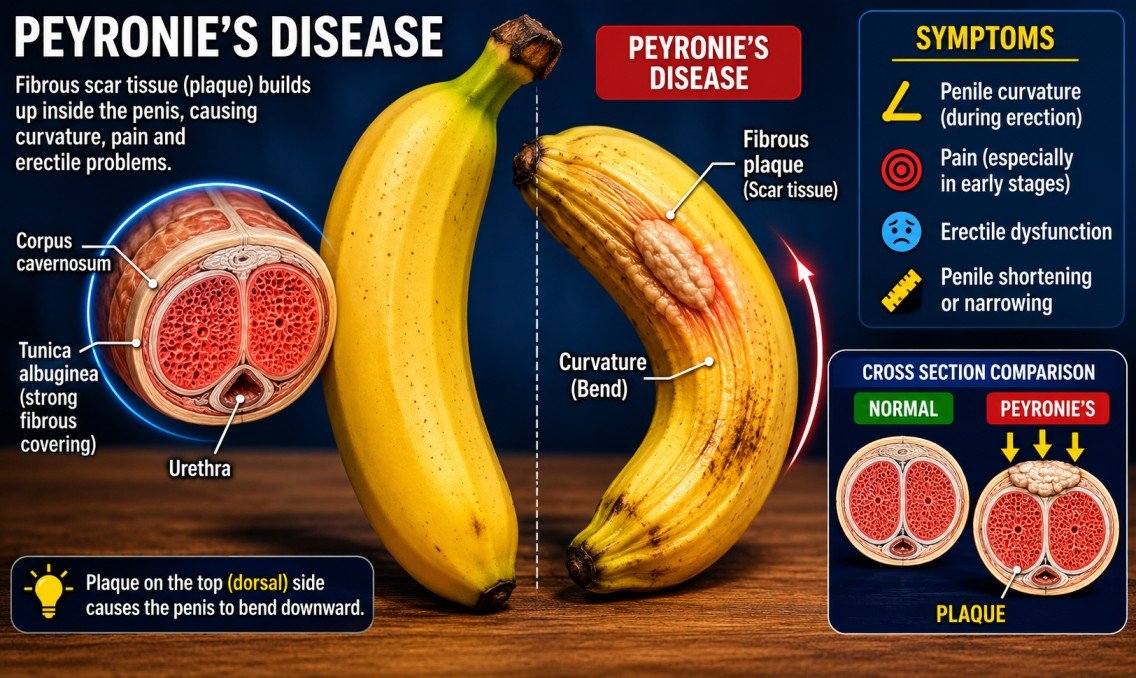
Peyronie’s disease is a condition that many men quietly struggle with, often avoiding conversations about it because of embarrassment or fear. Yet the condition is far more common than most people realize. Studies suggest that approximately 1 in 10 men may experience some degree of Peyronie’s disease during their lifetime, although many cases likely go unreported. The condition occurs when fibrous scar tissue, also called plaque, develops under the skin of the penis. This buildup can cause curvature, pain, shortening, and difficulties with erections.
For some men, the curvature is mild and manageable. For others, it can become severe enough to interfere with intimacy and everyday confidence. Imagine trying to bend a flexible straw that has a hardened knot in the middle. Instead of curving naturally, the straw twists awkwardly and resists movement. That is similar to what happens inside penile tissue when scar tissue forms.
Peyronie’s disease typically develops in two stages. The first is the acute phase, where pain and curvature gradually worsen over several months. The second is the chronic phase, where the condition stabilizes but the deformity remains. Some men also experience narrowing, indentation, or an “hourglass” appearance during erections.
What makes Peyronie’s disease particularly difficult is that it rarely affects only physical health. It can impact self-esteem, sexual relationships, and emotional well-being. Many men report anxiety, depression, or avoidance of intimacy because they fear judgment or disappointment. Understanding the available treatments—including newer regenerative therapies like the P-Shot and traditional surgical procedures—is often the first step toward regaining confidence and sexual function.
What Causes Peyronie’s Disease?
Doctors still do not fully understand why Peyronie’s disease develops, but most experts believe repeated penile trauma plays a major role. These injuries may happen during sexual activity, sports, accidents, or even minor unnoticed bending over time. In some men, the body heals normally after injury. In others, excessive scar tissue forms and hardens.
Genetics may also increase the risk. Men with connective tissue disorders such as Dupuytren’s contracture appear more likely to develop Peyronie’s disease. Age is another factor because tissue elasticity decreases as men grow older. Reduced blood circulation and slower healing may make scar formation more likely.
Certain lifestyle habits can contribute as well. Smoking, diabetes, high blood pressure, and poor cardiovascular health can damage blood vessels and tissue repair mechanisms. This is one reason many urologists emphasize overall health improvement alongside Peyronie’s treatment. Healthy circulation supports healing and sexual performance.
Psychological stress can also intensify symptoms. While stress does not directly cause Peyronie’s disease, anxiety may worsen erectile dysfunction and create tension during intimacy. Men who become fearful of pain or embarrassment sometimes avoid sexual activity altogether, creating additional emotional strain.
One challenge in diagnosing Peyronie’s disease is that symptoms vary significantly between individuals. Some men notice only a slight curve, while others experience severe bending exceeding 60 degrees. The degree of curvature often influences whether doctors recommend conservative therapies like the P-Shot or more invasive surgical correction.
Common Symptoms Men Experience
The most recognizable symptom of Peyronie’s disease is penile curvature during erection. The bend may point upward, downward, or sideways depending on where the scar tissue develops. In some cases, the penis may appear shortened or narrowed. Men often notice a hard lump or plaque beneath the skin, which can feel uncomfortable when touched.
Pain is especially common during the early inflammatory stage. Some men describe a dull ache, while others experience sharp discomfort during erections. The pain may eventually improve even if the curvature remains. Erectile dysfunction is another major symptom because scar tissue can interfere with blood flow and normal tissue expansion.
Sexual performance and confidence often decline alongside physical symptoms. Men may become anxious about intimacy or avoid relationships entirely. Research published in the Journal of Sexual Medicine found that emotional distress affects a substantial percentage of Peyronie’s patients, with many reporting depression and relationship strain.
Another frustrating symptom is unpredictability. Peyronie’s disease can progress slowly or rapidly, and no two cases are exactly alike. Some men see stabilization after several months, while others continue experiencing worsening curvature over time. This uncertainty is one reason treatment decisions can feel overwhelming.
The severity of symptoms usually determines which therapies are most appropriate. Mild cases may respond to non-invasive treatments such as traction therapy, medications, or the P-Shot, while severe structural deformities often require surgery to restore function.
Why Peyronie’s Disease Impacts More Than Physical Health
Peyronie’s disease is often discussed as a structural condition, but its emotional impact can be equally devastating. Sexual health is deeply connected to identity, confidence, and relationships. When a man suddenly experiences curvature, pain, or erectile dysfunction, the emotional effects can ripple through every aspect of life.
Many men feel isolated because they believe they are alone in facing the condition. Some avoid discussing it even with partners or healthcare providers. This silence can create shame and worsen anxiety. A man who once felt confident in intimate situations may begin overthinking every interaction. The fear of rejection can become more painful than the physical symptoms themselves.
Relationships may also suffer. Communication often breaks down when intimacy becomes stressful or uncomfortable. Partners may misinterpret avoidance as emotional distance rather than physical insecurity. Without open discussion, misunderstandings can grow. This is why many specialists encourage couples to approach Peyronie’s disease as a shared challenge rather than an individual problem.
Mental health concerns are surprisingly common among Peyronie’s patients. Studies have linked the condition to increased rates of depression and lowered quality of life. Men sometimes become trapped in a cycle where stress worsens erectile difficulties, and erectile difficulties increase stress. The emotional burden can affect work performance, social interactions, and overall well-being.
Treatment decisions are often influenced by these psychological factors. Some men prefer the P-Shot because it feels less invasive and more natural, while others choose surgery because they want a faster and more dramatic correction. Neither decision is purely medical. Emotional comfort, lifestyle, expectations, and relationship dynamics all play a role.
Emotional and Relationship Challenges
The emotional toll of Peyronie’s disease is frequently underestimated. Men may struggle with body image issues similar to those experienced in other chronic health conditions. Looking in the mirror or anticipating intimacy can trigger frustration, embarrassment, or sadness.
Partners are affected too. A healthy sexual relationship often relies on mutual confidence and communication. When one partner begins withdrawing due to Peyronie’s disease, emotional intimacy may decline as well. Some couples stop talking openly about sex altogether because the topic feels uncomfortable.
Counseling can sometimes help alongside medical treatment. Therapists specializing in sexual health can provide tools for communication, anxiety reduction, and rebuilding intimacy. Support groups also help many men realize they are not alone.
Interestingly, treatment success is not measured only by physical straightening. Patient satisfaction often depends just as much on restored confidence and emotional relief. A man who regains comfort during intimacy may consider treatment successful even if a slight curve remains.
This broader perspective is important when comparing P-Shot vs surgery for Peyronie’s disease. Surgery may deliver more noticeable structural correction, but the P-Shot may appeal to men seeking a gentler approach with less downtime and psychological stress.
Traditional Treatment Options for Peyronie’s Disease
Before regenerative therapies like the P-Shot gained attention, Peyronie’s disease treatment focused mainly on medications, injections, traction devices, and surgery. Each option has different goals, risks, and success rates. The right choice often depends on the severity of curvature, erectile function, and how long symptoms have been present.
Doctors usually begin with conservative treatment during the early stages of Peyronie’s disease. Oral medications such as pentoxifylline or vitamin E have been used, although evidence for their effectiveness remains mixed. Injectable medications, particularly collagenase clostridium histolyticum (Xiaflex), are more widely supported by clinical research. Xiaflex works by breaking down collagen in the plaque, potentially reducing curvature over time.
Traction therapy is another non-surgical option. Devices gently stretch the penis over several months to improve curvature and length. While the process requires patience and consistency, some men achieve measurable improvement without surgery.
Shockwave therapy has also emerged as a treatment option, especially for pain reduction. Low-intensity sound waves may stimulate tissue healing and improve blood flow. Results vary, but some men experience symptom relief.
Despite these alternatives, surgery remains the gold standard for severe Peyronie’s disease, especially when curvature prevents intercourse or causes major deformity. Surgical correction tends to provide the most immediate structural improvement, though it also carries greater risks and recovery time.
The rise of the P-Shot, which uses platelet-rich plasma (PRP), has introduced a newer category of regenerative medicine into Peyronie’s treatment discussions. Advocates believe PRP may support tissue healing and improve erectile quality, though scientific evidence is still evolving compared to established surgical methods.
Medications and Non-Surgical Therapies
Non-surgical treatments are often the first line of defense for men dealing with Peyronie’s disease, especially during the early inflammatory stage. Doctors usually prefer conservative methods before recommending surgery because many men either have mild curvature or want to avoid invasive procedures. These treatments aim to reduce pain, improve erectile function, and prevent the condition from worsening. While they may not completely eliminate curvature in every case, they can significantly improve quality of life when used consistently and under medical supervision.
One of the most recognized FDA-approved treatments is Xiaflex, an injectable medication designed to break down collagen buildup inside the plaque. The treatment involves a series of injections directly into the scar tissue, followed by penile modeling exercises performed by a doctor and the patient at home. Clinical studies have shown that Xiaflex can reduce curvature by approximately 30% to 35% in suitable candidates. That may not sound dramatic at first glance, but for many men, even a moderate reduction can make intercourse more comfortable and restore confidence.
Penile traction therapy is another increasingly popular non-surgical option. It works almost like physical therapy for the penis. Patients wear a traction device for a specified number of hours daily over several months. The gentle stretching encourages tissue remodeling and may improve both curvature and penile shortening. Consistency is crucial here. Men who stick with the treatment schedule tend to report better outcomes than those who use the device irregularly.
Oral medications have produced mixed results. Some doctors prescribe pentoxifylline to reduce inflammation and prevent calcification of plaque, while antioxidants like vitamin E are sometimes used despite limited evidence. Low-intensity shockwave therapy is another emerging approach that may reduce pain and stimulate blood flow, although its effect on curvature remains inconsistent in studies.
This landscape of conservative treatment created the foundation for newer regenerative therapies such as the P-Shot, which combines PRP technology with the body’s natural healing mechanisms. Many patients are drawn to the idea of improving symptoms without incisions, stitches, or lengthy downtime.
When Doctors Recommend Surgery
Surgery is usually considered when Peyronie’s disease becomes severe, stable, and disruptive to sexual function. Most urologists recommend waiting until the condition has stopped progressing for at least six to twelve months before considering an operation. Operating during the active inflammatory phase may increase the risk of recurrence or unpredictable results.
Men who experience severe curvature—typically over 60 degrees—or major deformities like indentation and narrowing are often surgical candidates. Surgery is also recommended when non-surgical therapies fail to improve symptoms or when intercourse becomes physically impossible. In cases where erectile dysfunction accompanies Peyronie’s disease and does not respond to medication, surgical intervention may offer the most reliable solution.
The decision to undergo surgery is highly personal. Some men prioritize rapid correction and are willing to accept surgical risks for a straighter erection. Others hesitate because of concerns about penile shortening, altered sensation, or recovery time. A skilled urologist usually evaluates several factors before recommending surgery, including erectile quality, plaque location, degree of curvature, and overall health.
There are three primary surgical approaches: plication surgery, plaque incision with grafting, and penile implants. Each procedure addresses Peyronie’s disease differently. Plication works by shortening the opposite side of the penis to straighten the curve. Grafting removes or cuts the plaque and places tissue grafts to restore shape. Penile implants are mainly reserved for men with significant erectile dysfunction alongside Peyronie’s disease.
One reason surgery remains highly respected is its predictability. Compared to experimental or regenerative treatments, surgery often produces more immediate and measurable straightening. However, the trade-off is greater invasiveness. Recovery may involve discomfort, temporary sexual restrictions, and the possibility of complications.
This is exactly why the comparison between P-Shot vs surgery for Peyronie’s disease has become such a major topic among patients. Men want to know whether they can avoid surgery while still achieving meaningful improvement.
What Is the P-Shot for Peyronie’s Disease?
The P-Shot, short for Priapus Shot, is a regenerative treatment that uses platelet-rich plasma (PRP) derived from the patient’s own blood. Although originally promoted for erectile dysfunction and sexual enhancement, some clinics now offer the P-Shot as a potential therapy for Peyronie’s disease. The treatment has gained attention because it is minimally invasive and relies on the body’s natural healing properties rather than surgical correction.
The process begins with a simple blood draw, similar to a routine lab test. The blood is then spun in a centrifuge to separate platelet-rich plasma from other blood components. PRP contains concentrated growth factors and proteins believed to support tissue repair, improve circulation, and stimulate cellular regeneration. Once prepared, the PRP is injected into targeted areas of the penis, including regions affected by Peyronie’s plaque.
Advocates of the P-Shot believe the treatment may help soften scar tissue, improve blood flow, and enhance erectile quality. Some men also report increased sensitivity and firmer erections after treatment. The concept behind PRP therapy is similar to regenerative techniques used in sports medicine, where athletes receive PRP injections to accelerate healing in injured tendons or joints.
One reason the P-Shot has become popular is its simplicity. The entire procedure usually takes less than an hour and is performed in an outpatient setting. Since the PRP comes from the patient’s own blood, the risk of allergic reaction is extremely low. Most men can resume normal activities within a day or two.
Still, the treatment remains somewhat controversial in the medical community. While anecdotal reports and smaller studies suggest potential benefits, large-scale clinical evidence for Peyronie’s disease specifically is still limited. Some urologists consider PRP promising but experimental, especially compared to established treatments like surgery or FDA-approved injections.
How the P-Shot Works
The science behind the P-Shot revolves around the regenerative power of platelets. Platelets are best known for helping blood clot after an injury, but they also release growth factors that support tissue repair and cellular communication. By concentrating these platelets and injecting them into damaged tissue, doctors hope to stimulate healing responses within the penis.
For Peyronie’s disease, the goal is not simply cosmetic straightening. The P-Shot aims to improve the quality of penile tissue itself. Scar tissue in Peyronie’s disease reduces elasticity and restricts blood flow during erections. PRP may encourage healthier tissue remodeling and reduce inflammation, potentially leading to improved flexibility and function.
Some clinics combine the P-Shot with other therapies such as acoustic wave therapy, penile traction, or vacuum erection devices. The idea is to create a more comprehensive regenerative environment. For example, traction therapy may physically stretch tissue while PRP supports cellular repair.
Patients usually receive local numbing cream or anesthetic injections before the procedure, making discomfort relatively mild. Most men describe the treatment as tolerable and quick. Unlike surgery, there are no incisions, sutures, or hospitalization requirements.
Results vary widely. Some men report noticeable improvements within weeks, while others require multiple sessions or see minimal changes. Experts generally agree that the P-Shot may be more effective in mild to moderate Peyronie’s disease rather than severe structural deformities.
The treatment’s growing popularity reflects a broader trend toward regenerative medicine. Many patients today prefer minimally invasive procedures whenever possible. Instead of cutting away tissue, regenerative approaches aim to encourage the body to repair itself naturally.
PRP Therapy Explained
PRP therapy has become one of the fastest-growing areas in regenerative medicine over the past decade. It is used in orthopedic medicine, dermatology, sports injury recovery, and cosmetic procedures. The principle is simple: use concentrated healing components from the patient’s own blood to support recovery in damaged tissue.
A standard PRP sample contains platelets at concentrations significantly higher than normal blood levels. These platelets release important growth factors such as platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), and vascular endothelial growth factor (VEGF). These compounds play critical roles in tissue repair, blood vessel formation, and collagen regulation.
In Peyronie’s disease, researchers believe PRP may help by improving circulation and reducing inflammation within fibrotic tissue. Better blood flow may also support stronger erections, which is particularly important because Peyronie’s disease often overlaps with erectile dysfunction.
Critics point out that PRP protocols vary dramatically between clinics. Different centrifuge methods, injection techniques, and treatment schedules make standardization difficult. This inconsistency partly explains why scientific evidence remains mixed. Some studies show encouraging improvements, while others find only modest benefits.
Despite the debate, patient interest continues growing. Many men are attracted to the idea of using their body’s own biology instead of synthetic medications or surgery. PRP also appeals to men who are not ready for permanent surgical intervention or who want to explore conservative treatments first.
The key takeaway is that the P-Shot is not necessarily a replacement for surgery in severe Peyronie’s disease. Instead, it may serve as an alternative or complementary therapy for selected patients seeking a less invasive path.
Benefits of the P-Shot for Peyronie’s Disease
One of the biggest advantages of the P-Shot is its minimally invasive nature. For many men, the idea of surgery on such a sensitive part of the body feels intimidating. The P-Shot offers a different experience entirely—no operating room, no general anesthesia, and no surgical incisions. That alone makes it attractive to patients who are hesitant about traditional procedures.
Recovery is typically much easier compared to surgery. Most men return to work and daily activities almost immediately after treatment. Mild swelling or bruising may occur temporarily, but serious complications are uncommon. This convenience appeals especially to busy professionals or men who cannot afford extended downtime.
Another potential benefit is improved erectile function. Peyronie’s disease often affects blood flow and erection quality. Since PRP may stimulate vascular regeneration, some patients report firmer erections and increased sensitivity after treatment. For men whose primary concern is erectile quality rather than severe curvature, this can be a meaningful improvement.
The P-Shot may also help preserve penile length. Surgical correction, particularly plication procedures, sometimes shortens the penis slightly because the longer side is tightened to match the scarred side. Regenerative therapies focus on tissue healing rather than structural shortening, which some patients see as a major advantage.
Psychologically, the treatment feels less aggressive. Men who fear surgery often experience relief knowing they can explore a lower-risk option first. This emotional comfort matters more than many people realize. Medical decisions are rarely based only on statistics; personal comfort and confidence play huge roles.
Cost and accessibility vary widely depending on location and clinic reputation. Since the P-Shot is often considered elective or experimental, insurance may not cover it. Still, some men prefer paying for regenerative therapy before committing to surgery.
The treatment may be especially beneficial for:
- Men with mild to moderate curvature
- Patients in earlier stages of Peyronie’s disease
- Men with erectile dysfunction alongside Peyronie’s
- Patients seeking non-surgical approaches
- Individuals wanting minimal recovery time
Minimally Invasive Nature
The minimally invasive nature of the P-Shot is one of the strongest reasons many men explore it before considering surgery. Traditional Peyronie’s procedures involve cutting, suturing, or implanting devices inside delicate penile tissue. Even when performed by experienced surgeons, surgery still places stress on the body and requires recovery time. The P-Shot, by comparison, feels much closer to a routine medical procedure than an operation.
The treatment is usually completed in under an hour at an outpatient clinic. Patients arrive, have a small blood sample drawn, and receive numbing medication before the PRP injections begin. There is no hospital admission and no need for general anesthesia. This streamlined process can dramatically reduce anxiety for men who feel overwhelmed by the idea of surgery.
Another major advantage is the lower risk profile. Because PRP comes from the patient’s own blood, allergic reactions and rejection issues are extremely rare. Surgical complications such as infection, scarring, or anesthesia-related risks are also largely avoided. Men who have underlying health concerns like diabetes or cardiovascular disease may appreciate having a less physically demanding option available.
The P-Shot also avoids permanent anatomical changes. Surgical correction physically alters penile structure, while PRP therapy attempts to support healing and tissue regeneration. Some men prefer this approach because it feels more natural and reversible. If the results are not satisfactory, surgery can still remain an option later.
From a lifestyle perspective, minimally invasive treatments fit modern expectations. Many patients today seek procedures with little interruption to work, family responsibilities, or exercise routines. The ability to receive treatment and resume normal life quickly makes the P-Shot especially appealing for active individuals.
That said, “minimally invasive” does not automatically mean “equally effective” for every case. Men with severe curvature or extensive plaque may still require surgery for meaningful correction. The P-Shot’s strength lies in its gentler approach, not necessarily in dramatic structural transformation.
Recovery Time and Comfort
Recovery is one area where the P-Shot clearly differs from surgery. Most men experience only mild discomfort after treatment, often described as temporary soreness or minor swelling. Bruising around injection sites may occur but typically fades within a few days. Patients can usually return to work immediately and resume light activities the same day.
Contrast that with surgical recovery, which can involve several weeks of healing. Men undergoing Peyronie’s surgery often need temporary restrictions on sexual activity, physical exercise, and heavy lifting. Swelling and discomfort are more pronounced after surgery, and some procedures require catheter use or postoperative bandaging.
The shorter recovery time associated with PRP therapy can reduce emotional stress as well. Many men feel more comfortable pursuing treatment when they know it will not significantly disrupt their daily lives. This convenience factor is especially important for patients balancing demanding careers or family responsibilities.
Pain management is generally simpler with the P-Shot too. Local anesthetic or numbing cream minimizes discomfort during the procedure itself. Most patients do not require prescription pain medication afterward. Surgical procedures, on the other hand, often involve postoperative pain management plans and careful monitoring during recovery.
Another overlooked advantage is discretion. Because there is little downtime, men can undergo treatment privately without explaining extended absences from work or social activities. For a condition already associated with embarrassment and stigma, that privacy matters.
Still, comfort and convenience must be balanced against expectations. The P-Shot may require multiple sessions for noticeable improvement, and results are not guaranteed. Surgery may involve more discomfort initially, but it often produces more immediate structural correction. Patients must decide whether they value quicker recovery or potentially stronger curvature correction more highly.
Risks and Limitations of the P-Shot
Although the P-Shot is often marketed as a revolutionary regenerative therapy, it is important to understand its limitations. One of the biggest concerns among medical professionals is the lack of large-scale standardized research specifically focused on Peyronie’s disease. While PRP therapy has shown promise in many areas of medicine, evidence regarding long-term outcomes for Peyronie’s remains limited.
Results can also be unpredictable. Some men report substantial improvements in curvature, erection quality, and sensitivity, while others notice only minor changes or none at all. Unlike surgery, which physically corrects deformity, PRP relies on biological healing responses that vary from person to person. Age, severity of plaque, circulation quality, and overall health can all influence results.
Another limitation is that the P-Shot may not adequately address severe curvature or calcified plaque. In advanced Peyronie’s disease, scar tissue can become dense and rigid, making regenerative therapy less effective. Men with extreme deformities may ultimately need surgery even after trying PRP treatments.
Cost is another factor. Since the P-Shot is often classified as elective or experimental, insurance coverage is uncommon. Patients may need multiple sessions, significantly increasing total expenses. Depending on the clinic, treatments can range from several hundred to several thousand dollars.
There is also variability in treatment quality between providers. PRP preparation methods differ widely, and not all clinics follow evidence-based protocols. Some providers market the P-Shot aggressively despite limited scientific support. Patients should carefully research practitioner credentials and seek experienced urologists or regenerative medicine specialists.
Potential side effects are generally mild but still possible. Temporary bruising, swelling, tenderness, or minor bleeding may occur. Infection risk is low but not impossible. Men should also be cautious of unrealistic claims promising dramatic enlargement or guaranteed cures.
Who May Not Be a Good Candidate?
Not every patient with Peyronie’s disease is an ideal candidate for the P-Shot. Men with severe penile curvature, extensive calcification, or significant structural deformities may not experience meaningful correction from PRP therapy alone. In these cases, surgery often remains the more reliable option.
Patients with uncontrolled diabetes, bleeding disorders, or active infections may also face increased risks or reduced effectiveness. Since PRP depends on healthy healing mechanisms, men with poor circulation or compromised immune function may not respond as well.
Expectations matter too. Men hoping for immediate dramatic straightening may feel disappointed with regenerative therapy. The P-Shot generally works gradually, and improvements may be subtle rather than transformative. Patients seeking guaranteed structural correction are often better served by surgical consultation.
Psychological readiness is another important consideration. Some men pursue experimental treatments out of desperation while avoiding difficult conversations about surgery. A realistic understanding of potential outcomes is essential before investing time and money into PRP therapy.
A thorough evaluation by a qualified urologist helps determine whether the P-Shot is appropriate. In many cases, doctors recommend combining treatments rather than relying on a single therapy. PRP may complement traction devices, medications, or shockwave therapy as part of a broader treatment plan.
Surgical Options for Peyronie’s Disease
Surgery has long been considered the most effective treatment for severe Peyronie’s disease. While non-surgical therapies may improve mild to moderate cases, surgery remains the gold standard when curvature significantly interferes with sexual function. Modern surgical techniques can dramatically straighten the penis and restore usability, though each method carries unique risks and trade-offs.
The type of surgery chosen depends on several factors:
- Degree of curvature
- Erectile function
- Plaque size and location
- Penile length
- Patient expectations
Doctors usually recommend surgery only after Peyronie’s disease has stabilized. This means the curvature has remained unchanged for several months and pain has mostly resolved. Operating too early may increase the chance of recurrence or unpredictable healing.
The three primary surgical approaches are:
- Plication surgery
- Plaque incision or excision with grafting
- Penile implants
Each procedure serves different patient needs. Men with good erectile function and moderate curvature often undergo plication. Patients with more severe deformities or narrowing may require grafting. Men struggling with both Peyronie’s disease and severe erectile dysfunction may benefit most from penile implants.
Surgery offers one major advantage over regenerative treatments like the P-Shot: predictability. Structural correction is usually immediate and measurable. Many patients achieve substantial straightening after a single procedure.
However, surgery is not without compromise. Potential downsides include penile shortening, altered sensation, erectile dysfunction, scarring, and recovery time. Choosing surgery requires careful discussion between patient and surgeon regarding expectations and risks.
Plication Surgery
Plication surgery is one of the most common procedures for Peyronie’s disease. The concept is surprisingly straightforward. Instead of removing the plaque, the surgeon shortens the longer side of the penis opposite the curvature. This creates a straighter erection by balancing both sides.
The procedure is typically recommended for men with:
- Curvature under 60 degrees
- Adequate penile length
- Good erectile function
- Minimal complex deformities
One reason plication remains popular is its relatively high success rate. Studies often report curvature improvement in over 80% to 90% of patients. The surgery is generally less invasive than grafting procedures and carries lower risks of postoperative erectile dysfunction.
Recovery tends to be quicker compared to more complex surgeries. Most men return home the same day and resume normal activities within a few weeks. Sexual activity is usually restricted temporarily while healing occurs.
The biggest drawback is potential penile shortening. Since the longer side is tightened to match the shorter scarred side, some men notice reduced length after surgery. For patients already distressed about Peyronie’s-related shortening, this can be emotionally difficult.
Despite this concern, many patients remain highly satisfied because the procedure reliably improves function and straightness. In practical terms, a slightly shorter but functional penis may feel preferable to severe curvature preventing intercourse altogether.
Plaque Incision and Grafting
Plaque incision and grafting is generally reserved for more severe or complex Peyronie’s disease cases. Instead of simply tightening the opposite side, the surgeon cuts into or removes portions of the plaque and places a graft to restore shape and flexibility.
This approach is often recommended for:
- Curvature greater than 60 degrees
- Significant narrowing or hourglass deformities
- Men concerned about preserving length
One major advantage is that grafting can maintain or even restore penile length better than plication surgery. Since the scarred side is expanded rather than shortened, the penis may retain a more natural appearance.
The procedure is technically more demanding, however, and carries higher risks. Erectile dysfunction after surgery is more common because the operation involves deeper manipulation of penile tissue and blood vessels. Recovery may also take longer.
Patients considering grafting must weigh the benefits of improved shape and length preservation against the increased possibility of complications. Experienced surgeons carefully evaluate vascular health and erectile function before recommending this option.
Penile Implants
Penile implants are typically considered for men with Peyronie’s disease combined with severe erectile dysfunction that does not respond to medication. Inflatable implants are most commonly used because they provide rigidity while also helping straighten curvature internally.
The implant cylinders are placed inside the penis surgically. During inflation, the device creates an erection mechanically. In many cases, the implant alone significantly reduces curvature. Additional straightening procedures may be performed simultaneously if necessary.
Satisfaction rates for penile implants are often very high, especially among men who struggled with both deformity and erectile dysfunction for years. Restoring dependable sexual function can dramatically improve confidence and relationships.
The downside is permanence. Implant surgery irreversibly changes erectile mechanics, and future natural erections are no longer possible. Risks include infection, mechanical malfunction, and surgical complications.
For the right patient, however, penile implants can feel life-changing. Men who once avoided intimacy because of pain, curvature, and erection failure may regain a satisfying sex life after treatment.
Benefits of Surgery for Peyronie’s Disease
The biggest strength of surgery is its effectiveness. Unlike conservative therapies that may produce gradual or modest improvement, surgery often provides immediate and significant straightening. For men with severe Peyronie’s disease, this can restore sexual function far more reliably than non-invasive alternatives.
Surgical outcomes are also more predictable. While regenerative treatments like the P-Shot depend heavily on individual healing responses, surgery directly changes penile structure. Patients and surgeons can often estimate expected correction more accurately.
Another benefit is durability. Surgical correction generally produces long-lasting results once healing is complete. Although recurrence is possible, many men maintain improvement for years.
Psychological relief can be enormous as well. Men who have struggled with embarrassment, avoidance of intimacy, or failed conservative treatments often experience renewed confidence after successful surgery. Relationships may improve alongside physical function.
For severe cases, surgery may simply be the only practical option. Dense plaque, major curvature, and advanced deformities often cannot be adequately corrected through injections or PRP therapy alone.
The comparison between P-Shot vs surgery for Peyronie’s disease ultimately comes down to balancing invasiveness against effectiveness. The P-Shot offers lower downtime and gentler treatment, while surgery delivers stronger and more predictable structural correction.
Risks and Side Effects of Surgery
While surgery can be highly effective for Peyronie’s disease, it is not without significant risks. Every surgical procedure involves a balance between potential benefits and possible complications, and penile surgery naturally carries emotional weight because of the organ involved. Understanding these risks honestly helps patients make informed decisions rather than choosing treatment based purely on fear or marketing claims.
One of the most common concerns is penile shortening. This is especially associated with plication surgery, where the longer side of the penis is tightened to create straightness. Even though the penis may function better afterward, some men feel distressed by reduced length. Since Peyronie’s disease itself can already shorten the penis, any additional reduction may affect confidence.
Erectile dysfunction is another potential complication. Procedures involving plaque incision and grafting carry a higher risk because they manipulate deeper tissue structures and blood vessels. Some men who had normal erections before surgery may experience weaker erectile function afterward. The risk varies depending on age, vascular health, surgical technique, and surgeon experience.
Changes in penile sensation can also occur. Temporary numbness is relatively common during healing, though permanent sensory changes are less frequent. Scar formation, infection, bleeding, and anesthesia-related complications are additional possibilities, although serious complications are uncommon when surgery is performed by an experienced reconstructive urologist.
Recovery can also test patience. Swelling, bruising, discomfort, and temporary restrictions on sexual activity are part of the healing process. Men often need several weeks before resuming intercourse. Emotional adjustment may take even longer, especially if expectations were unrealistic beforehand.
Another challenge is that no surgery guarantees perfection. Some degree of residual curvature may remain, particularly in severe cases. Patients hoping for a completely flawless result can feel disappointed even when the procedure is medically successful.
This is why expert consultation matters so much. A qualified specialist does more than explain surgical techniques—they help patients develop realistic expectations. Men who understand both the strengths and limitations of surgery tend to report higher satisfaction afterward.
P-Shot vs Surgery: Key Differences
The debate between P-Shot vs surgery for Peyronie’s disease comes down to one central question: does a patient prioritize minimally invasive treatment or maximum structural correction? Both approaches have advantages, but they serve very different patient needs.
The P-Shot focuses on regeneration and healing. It aims to improve tissue quality, circulation, and erectile function using platelet-rich plasma derived from the patient’s own blood. Surgery, on the other hand, physically reshapes or reconstructs the penis to correct curvature directly.
Think of it like repairing a damaged tree branch. The P-Shot attempts to nourish and strengthen the branch naturally over time, while surgery cuts and reshapes the branch immediately. Neither approach is universally “better.” The ideal treatment depends on severity, expectations, health status, and personal comfort.
Men with mild to moderate Peyronie’s disease often prefer the P-Shot because it avoids incisions, anesthesia, and lengthy recovery. Patients with severe curvature or major deformities may require surgery because regenerative therapy alone may not produce enough structural improvement.
Cost, downtime, predictability, and emotional comfort also differ significantly. Surgery typically delivers faster and more dramatic results but comes with greater risks. The P-Shot offers convenience and lower recovery demands but less certainty regarding outcomes.
Another major distinction is scientific evidence. Surgical techniques have decades of clinical research supporting them, while PRP-based treatments still require larger standardized studies. This does not mean the P-Shot lacks value, but patients should recognize the difference between established surgical data and emerging regenerative medicine trends.
Effectiveness
When it comes to pure curvature correction, surgery generally outperforms the P-Shot. Procedures such as plication and grafting can produce substantial straightening immediately after healing. Success rates for surgical correction often exceed 80%, especially when performed by experienced specialists.
The P-Shot may improve curvature modestly in selected patients, but results vary widely. Some men experience softer plaque, improved flexibility, and better erections, while others notice little structural change. PRP appears most effective in mild to moderate cases rather than severe deformities.
Effectiveness also depends on treatment goals. If a man’s main concern is erectile quality or circulation, the P-Shot may provide meaningful improvement even if curvature remains partially unchanged. Surgery focuses more on physical straightness and functional intercourse capability.
Combination therapy is becoming increasingly common as well. Some doctors integrate PRP with traction therapy, shockwave treatment, or postoperative healing protocols. Rather than viewing the P-Shot and surgery as direct competitors, some specialists see them as complementary tools.
Cost Comparison
Cost is another major consideration. Peyronie’s surgery can be expensive, particularly when hospital fees, anesthesia, and specialist care are included. Insurance may cover medically necessary procedures, especially when curvature significantly interferes with sexual function.
The P-Shot often falls into a gray area because many insurers classify it as elective or experimental. Patients frequently pay out of pocket. Depending on the clinic and geographic location, one session may cost anywhere from several hundred to several thousand dollars. Multiple treatments may also be recommended.
Ironically, some patients spend substantial amounts on repeated regenerative treatments before eventually pursuing surgery anyway. Others feel the lower upfront commitment of PRP therapy is worth trying before considering an operation.
Financial decisions should include more than procedure costs alone. Recovery time, missed work, follow-up appointments, and emotional stress all contribute to the overall burden of treatment.
Recovery and Downtime
Recovery differences between the two treatments are dramatic. The P-Shot usually allows patients to resume normal routines within a day or two. Mild soreness or bruising is common but generally short-lived. There are no incisions, stitches, or hospitalization requirements.
Surgery involves a much longer healing process. Patients may experience swelling, pain, and temporary limitations on physical activity and intercourse. Full recovery can take several weeks or even months depending on the procedure.
For busy individuals or men unwilling to pause daily responsibilities, the P-Shot’s convenience can be highly attractive. Others may willingly accept surgical downtime if it means achieving more reliable correction.
The psychological aspect of recovery also matters. Some men feel emotionally drained after surgery because healing is slower and more physically demanding. Minimally invasive therapies may feel less intimidating and easier to process mentally.
Long-Term Results
Long-term outcomes remain one of the strongest arguments for surgery. Surgical correction has decades of data supporting durable improvements in penile straightness and function. While recurrence can occur, many men maintain results for years.
The long-term effectiveness of PRP therapy for Peyronie’s disease is less established. Since the treatment is relatively new in this field, research is still evolving. Some men report lasting benefits, while others require repeat sessions to maintain improvements.
This uncertainty does not automatically make the P-Shot ineffective. Regenerative medicine is advancing rapidly, and future studies may strengthen its credibility. For now, however, surgery remains the more evidence-backed option for severe Peyronie’s disease.
Which Treatment Is Better for Different Patients?
There is no universal answer to whether the P-Shot or surgery is “better.” The best treatment depends entirely on the patient’s condition, goals, risk tolerance, and expectations.
The P-Shot may be better suited for:
- Men with mild to moderate curvature
- Patients seeking non-invasive treatment
- Men with erectile dysfunction alongside Peyronie’s
- Individuals wanting minimal downtime
- Patients interested in regenerative therapies
Surgery may be better suited for:
- Severe curvature preventing intercourse
- Significant penile deformity or shortening
- Calcified plaque
- Men wanting immediate structural correction
- Patients who failed conservative treatments
Age and overall health matter too. Younger men with early-stage Peyronie’s disease may prefer trying regenerative approaches first. Older patients with advanced plaque and severe dysfunction may achieve better outcomes surgically.
Personality also influences treatment satisfaction more than many people expect. Some men value certainty and decisive correction, making surgery emotionally reassuring despite the risks. Others prioritize safety, comfort, and gradual healing, making the P-Shot more appealing.
An experienced urologist should guide this decision through a personalized evaluation rather than a one-size-fits-all recommendation. Peyronie’s disease varies enormously from person to person, and treatment should reflect that individuality.
Questions to Ask Your Doctor Before Choosing Treatment
Before deciding between the P-Shot and surgery, patients should have a detailed conversation with a qualified urologist. Asking the right questions can prevent disappointment and clarify expectations.
Important questions include:
- How severe is my curvature?
- Is my Peyronie’s disease stable yet?
- What results can realistically be expected?
- What are the risks of each treatment option?
- Will I likely need multiple procedures?
- How might treatment affect penile length and sensation?
- What is the recovery timeline?
- Are there non-surgical alternatives worth trying first?
- How experienced are you with this procedure?
- What do long-term outcomes typically look like?
Patients should also ask to see before-and-after examples when appropriate. Realistic visual outcomes often communicate more effectively than vague promises.
Another valuable step is seeking a second opinion. Peyronie’s disease treatment can vary widely between providers, especially in clinics heavily marketing regenerative therapies. A balanced perspective helps patients avoid rushing into unnecessary procedures.
Conclusion
Choosing between the P-Shot vs surgery for Peyronie’s disease is ultimately about balancing goals, risks, and expectations. The P-Shot offers a minimally invasive regenerative approach with little downtime and potential improvements in erectile quality and tissue health. Surgery provides stronger and more predictable structural correction, especially for severe curvature and advanced disease.
Neither treatment is perfect for every patient. Men with mild to moderate symptoms may appreciate the convenience and lower risk profile of PRP therapy. Those facing severe deformity, painful intercourse, or major functional limitations often achieve better results surgically.
The most important step is seeking evaluation from a qualified specialist who understands both regenerative medicine and reconstructive urology. Peyronie’s disease affects far more than physical appearance—it impacts confidence, relationships, and emotional well-being. The right treatment should address all of those dimensions, not just curvature alone.
With modern advancements in both surgery and regenerative therapies, men today have more options than ever before. Whether choosing the P-Shot, surgery, or a combination approach, informed decision-making offers the best path toward restoring comfort, function, and confidence.